Amsterdam, Netherlands – 28 Aug 2023: Active screening of patients with type 2 diabetes or chronic obstructive pulmonary disease (COPD) more than doubles new diagnoses of cardiovascular disease compared with usual care, according to late breaking research presented in a Hot Line session today at ESC Congress 2023.1
Coronary artery disease, atrial fibrillation and heart failure are chronic progressive conditions affecting millions of people worldwide and leading to significant morbidity, mortality and healthcare costs. Early stages of these diseases usually manifest with nonspecific symptoms in primary care, rather than in hospitals. Treatments are available that may prevent acute events, such as acute myocardial infarction, stroke or acute heart failure. Screening has therefore been proposed as a potential strategy to identify patients and expedite timely management. However, despite the large overlap in risk factors, sign and symptoms, previous screening studies have targeted each disease separately,2-6 and systematic screening is not common practice. Thus, there is an urgent need for a primary care strategy aimed at uncovering all three cardiac diseases in groups at high risk of cardiovascular disease, such as those with COPD or type 2 diabetes.
RED-CVD was a cluster randomised, pragmatic trial examining the ability of a stepwise diagnostic strategy to identify coronary artery disease, atrial fibrillation and heart failure in patients with COPD or type 2 diabetes using tools readily available in primary care.7 In the trial, primary care practices were the unit of randomisation. Primary care practices across the Netherlands were eligible if they could add the early diagnosis strategy to their usual disease management programmes for type 2 diabetes and COPD.
Between June 2019 and January 2023, 25 primary care practices were randomly allocated to the intervention arm or the control arm. The intervention had three steps: 1) a questionnaire on risk factors and symptoms, to be filled out at home prior to the next routine visit to a type 2 diabetes or COPD management programme; 2) for patients who scored above a prespecified threshold on the questionnaire: a physical examination by the practice nurse focused on signs of heart failure, 12-lead electrocardiography (ECG) and NT-proBNP measurements, to be performed during a routine visit; and 3) interpretation of the results of steps 1 and 2 by the GP and referral to a cardiologist or open access echocardiography if deemed necessary.
The primary outcome was a composite of newly detected cases of heart failure, atrial fibrillation and coronary artery disease at one year after the baseline visit. Secondary endpoints included newly initiated treatments at one year after the baseline visit.
The trial included 1,216 patients, of whom 87% had type 2 diabetes and 20% had COPD (few patients had both conditions). The average age of participants was 68 years and 40% were women. Regarding the primary outcome, during one year of follow-up, 50 of 624 participants (8.0%) in the intervention group and 19 of 592 participants (3.2%) in the control group were newly diagnosed with at least one of heart failure, atrial fibrillation or coronary artery disease (adjusted odds ratio 2.83; 95% confidence interval, 1.62 to 4.95). Heart failure was the most common new diagnosis (4.5% in the intervention group vs. 1.5% in the control group), followed by coronary artery disease (2.6% vs. 1.4%, respectively) and atrial fibrillation (2.1% vs. 1.0%, respectively).
Regarding the secondary endpoint of newly initiated treatments, no major differences in medication use at follow-up were observed between the intervention and control groups.
Study author Dr. Amy Groenewegen of the University Medical Centre Utrecht, the Netherlands said: “An easy-to-implement strategy more than doubled the number of new diagnoses of heart failure, atrial fibrillation and coronary artery disease in high-risk patients. Because there are so many adults in the community with COPD or type 2 diabetes, this approach could translate into tens of thousands of new diagnoses when applied at large. In the Netherlands, for example, screening the more than 920,000 patients with COPD and/or type 2 diabetes could identify over 44,000 patients with at least one previously undiagnosed cardiovascular condition (Figure 1).”
Figure 1: Potential for a new screening strategy to diagnose cardiac conditions
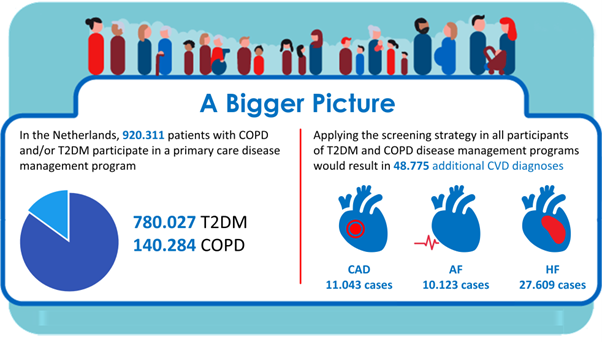
AF: atrial fibrillation;
ENDS